

On March 1, 2012 and May 1, 2012, several amendments were made to this protocol. To view these amendments, please see the section titled “Summary of Protocol Amendments.”
Background and Objectives for the Systematic Review
Coronary artery disease (CAD) is a leading cause of morbidity and mortality worldwide, accounting for 35 percent of all deaths in the United States and 30 percent of all deaths globally in 2005.1 The diagnosis of CAD is made on the basis of stenosis within one or more coronary epicardial arteries. Treatment options for CAD include medical therapy and invasive revascularization with either percutaneous coronary intervention (PCI) or bypass surgery. Clinical recommendations for revascularization have traditionally been based on qualitative and quantitative coronary angiography. While angiograms are still regarded as the reference standard for anatomic visualization of coronary arteries, they are not without limitation.
Coronary angiograms only visualize an outline of the luminal wall and are generally ineffective in determining the functional importance of stenoses. Angiographic evidence of stenosis is usually not detected until the plaque approaches 40 to 50 percent of the total cross-sectional area of the coronary artery, because the outer wall of the artery enlarges to accommodate the growing plaque (positive remodeling).2 Thus, for intermediate ranges of coronary stenoses (40 to 80 percent), there is considerable variability between physiologic and angiographic assessments of the severity of stenosis, often making it difficult to determine whether PCI is needed.3 In addition, most complex plaques do not reveal sufficient alterations by angiography, thereby limiting assessment of complex lesions with this technique (e.g., ostial, graft, or bifurcation lesions). Moreover, angiograms cannot provide information on the composition of the coronary plaque, which could be important in determining therapeutic choices.2
Several adjunctive intravascular diagnostic procedures and imaging techniques (collectively referred to as IVDx) have been developed for the purpose of providing more detailed anatomic and hemodynamic information. IVDx techniques do not preclude the need for angiography but rather are complementary in nature by assisting treatment decisionmaking.4
Among the IVDx imaging techniques used to visualize coronary anatomy, intravascular ultrasound (IVUS) is the most common. During PCI, IVUS provides high-resolution images of the vessel and lumen geometry and enables analysis of plaque composition and distribution, as well as guidance of coronary stent implantation. IVUS can also be used to quantitatively assess revascularization success or diagnose stent-related complications,5,6 but it does not directly measure the hemodynamic effects of a stenosis.
Fractional flow reserve (FFR), in contrast, is an IVDx technique used to determine the physiologic significance of a coronary stenosis. An FFR value <0.75 indicates inducible ischemia, 0.75–0.80 represents an intermediate “grey” zone, and a value >0.80 generally excludes ischemia related to a specific stenosis.3,7,8
Other IVDx techniques that are less widely used or are still evolving include coronary flow reserve (CFR), IVUS-virtual histology (VH-IVUS), integrated backscatter IVUS, optical coherence tomography (OCT), near-infrared spectroscopy, angioscopy, thermography, and intravascular magnetic resonance imaging (MRI).
IVDx techniques are potentially valuable in a number of clinical scenarios. For example, as previously described, IVUS provides precise visualization of intracoronary anatomy, atherosclerotic plaque composition, and changes in vessel dimensions. Its use could diagnose patients who have coronary stenoses that might otherwise be missed, thereby improving long-term clinical outcomes. Conversely, FFR might help identify patients whose stenoses are not really impeding flow and thereby reduce the number of unneeded stents and limit patient exposure to blood thinners and repeat revascularizations.
Nevertheless, these techniques remain invasive, and their application can result in procedure-related complications or increased procedural times and initial costs and possibly generate additional unnecessary invasive tests or unnecessary treatments that can adversely impact long-term clinical outcomes. Therefore, their use should be weighed by considering the potential benefit of the additional diagnostic information gained versus noninvasive alternatives. These decisions are not always straightforward. Other, noninvasive imaging techniques for evaluating stenoses (e.g., cardiac computed tomography) that are available have a much lower resolution than IVUS. Moreover, invasive techniques such as IVUS are able to detect plaques much earlier than cardiac MRI, that is before the plaques attain maximum maturity.9 In addition, available noninvasive methods are not also without their own associated adverse events, costs, and technology-specific risks (e.g., exposure to radiation). Thus, despite their potential drawbacks, invasive IVDx modalities have emerged as potentially important complementary tools to angiography.
Recent clinical practice guidelines have indicated that FFR and IVUS can be useful in certain clinical contexts—specifically, FFR in determining the necessity of PCI and IVUS for providing technical guidance during PCI and optimizing PCI results.10,11 However, the currently available guidelines and systematic reviews do not comprehensively examine the role of IVDx techniques in relation to the settings of interest and are not generally applicable to contemporary practice, as recent literature (e.g., for drug-eluting stents) has not yet been thoroughly reviewed. Furthermore, variation in how IVDx techniques are adopted in clinical practice across catheterization laboratories reflects considerable uncertainty about the utility and role of these techniques.12 Thus, a comparative effectiveness review on the use of IVDx applications in patients with CAD is timely and necessary to assess the clinical impact of incorporating such techniques into coronary catheterization procedures.
Key Questions
Response to Public Comments
The Key Questions (KQs) for our review were posted on the Effective Health Care Program Web site (http://effectivehealthcare.ahrq.gov) for public comment from March 22 to April 19, 2011. Public comments received through the Web site were considered in preparation of this protocol.
In response to a request to clarify the role of IVDx techniques in the choice of a specific PCI technique, we have defined the clinical context of each KQ and pointed out that KQ 2 would address this clinical question specifically. We do not plan to evaluate technical attributes of each technique, since the focus of our review will be assessment of clinical outcomes. Despite the potential lack of evidence on clinical outcomes, we will include all relevant KQs and identify future research needs when appropriate.
We plan to evaluate the impact of IVDx techniques on the diagnostic thinking of physicians. In defining the outcomes to be analyzed in our review, we provide explicit examples of the terms “diagnostic thinking” and the types of outcomes that fall under its formal definition in the evaluation of diagnostic tests.15
On the basis of input from Key Informants during the Topic Refinement phase, this review will not examine diagnostic test performance (e.g., sensitivity and specificity) for the following reasons:
- Other than FFR, whose diagnostic accuracy has been established in a previous meta-analysis,13 all other IVDx techniques concern the histopathological structure of lesions and thus require a histopathological specimen to confirm imaging findings.
- Based on a previous literature review,14 we identified that such literature is limited.
- Such an evaluation clearly falls outside the scope of our review, which is to evaluate the impact of the information provided by the application of IVDx techniques on a set of clinical outcomes.
Key Questions (KQ)
Our review will focus on the following five KQs:
- Key Question 1: For patients undergoing diagnostic coronary angiography to evaluate the presence/extent of CAD in order to decide on the necessity for coronary intervention, what is the impact of using an IVDx technique—when compared to angiography alone—on the diagnostic thinking and therapeutic decisionmaking, short-term outcomes, and long-term outcomes?
- Key Question 2: For patients undergoing PCI, what is the impact of using an IVDx technique to guide the PCI procedure (either immediately prior to or during the procedure)—when compared to angiography-guided PCI—on the diagnostic thinking and therapeutic decisionmaking, short-term outcomes, and long-term outcomes?
- Key Question 3: For patients having just undergone a PCI, what is the impact of using an IVDx technique to evaluate the success of PCI immediately after the procedure—when compared to angiography alone—on the diagnostic thinking and therapeutic decisionmaking, short-term outcomes, and long-term outcomes?
- Key Question 4: How do different IVDx techniques compare to each other in their effects on the diagnostic thinking and therapeutic decisionmaking, short-term outcomes, and long-term outcomes?
- During diagnostic coronary angiography for the evaluation of the presence/extent of CAD and the potential necessity of coronary intervention?
- During PCI to guide the procedure?
- Immediately after PCI to evaluate the success of PCI?
- Key Question 5: What factors (e.g., patient/physician characteristics, availability of prior noninvasive testing, type of PCI performed) influence the effect of IVDx techniques—when compared to angiography (or among different IVDx techniques)—on the diagnostic thinking and therapeutic decisionmaking, short-term outcomes, and long-term outcomes?
- During diagnostic coronary angiography for the evaluation of the presence/extent of CAD and the potential need for coronary intervention?
- During PCI to guide the procedure?
- Immediately after PCI to evaluate the success of PCI?
Eligibility Criteria
Eligible studies to be included in our review should fulfill the following inclusion criteria with respect to population, interventions, comparators, outcomes, timing, study designs, and settings (PICOTS).
Populations
- Adults (≥18 years)
- For KQs 1, 4a, and 5a: Patients who undergo diagnostic coronary angiography and are evaluated for the presence or extent of CAD in order to decide on the need for coronary intervention.
All patients considered to be candidates for coronary interventions can be evaluated on the basis of the following subgroups, as reported in individual studies:- Intermediate coronary stenoses (>40–50 percent and <70–80 percent), either ischemic or nonischemic
- Left main artery lesions
- Any type of complex coronary lesions (e.g., long diffuse lesions, tandem lesions, bypass conduit vessel lesions, bifurcation lesions, total occlusions, ostial lesions, stent thromboses, thrombotic and nonthrombotic lesions; in-stent restenosis; and those with stent fractures)
- Nonobstructive coronary lesions (e.g., vulnerable plaques)
- For KQs 2, 4b, and 5b: Patients who need PCI and are evaluated with an IVDx technique and/or angiography to guide the PCI procedure (either immediately before or during the procedure)
- For KQs 3, 4c, and 5c: Patients evaluated with an IVDx technique and/or angiography immediately after PCI (stent placement or other type of PCI) to evaluate the success of PCI (and the potential need for reintervention).
- Subgroups of interest for all KQs:
- Patients with different manifestations of CAD (ST segment elevation myocardial infarction [STEMI], non-STEMI, unstable angina, and stable angina)
- Patients who have diabetes and those who do not
- Patients with chronic inflammation (e.g., systemic lupus erythematosus)
- Patients who have atherosclerosis following a heart transplant
Interventions
- For all KQs: Intravascular diagnostic procedures that evaluate morphological or physiological parameters of coronary lesions:
- Interventions presently employed in clinical care, as recommended by technical expert panel:
- FFR
- IVUS
- Interventions that are mainly investigational at present:
- IVUS with virtual histology
- Optical coherence tomography
- Elastography
- Near-infrared spectroscopy
- Thermography
- Angioscopy
- Intravascular MRI
- Other indices such as stenosis index and index of microcirculatory resistance
- Interventions presently employed in clinical care, as recommended by technical expert panel:
Comparators
- For KQs 1–3 and 5: Conventional coronary angiography
- For KQs 4 and 5: Any index IVDX technique (for head-to-head comparisons)
Outcomes
Outcomes of interest are categorized into two types: diagnostic and treatment thinking outcomes and process and patient-centered outcomes.
Diagnostic thinking and therapeutic decisionmaking outcomes include:
- KQ1: During diagnostic workup of CAD, the change in the number of hemodynamically significant lesions after the application of IVDx, or the change in the decision about an interventional therapy (e.g., if PCI is needed) after the application of IVDx
- KQ2: During PCI, the change in the number of diagnoses of a complex lesion requiring additional intervention after the application of IVDx, or the change in the type of PCI treatment after the application of IVDx
- KQ3: Immediately after PCI, the change in the number of successful PCIs after the application of IVDx, or how frequently the decision about the need for reintervention planned before IVDx changed after the test
Process and patient-centered outcomes are further categorized into short-term outcomes and intermediate or long-term outcomes. They are as follows:
- Short-term (≤30 days) outcomes:
- In-hospital procedural outcomes
- Process outcomes (technical success rates assessed by quantitative coronary angiography [QCA], such as proportion of successful completion of attempted procedures or proportion of interpretable results in completed procedures, total procedural time required, fluoroscopy, and contrast agent exposure)
- Periprocedural complications (e.g., MI, death, vessel dissection, bleeding, repeat PCI, or bypass surgery)
- Stent-related complications (e.g., acute stent thrombosis, and dissection)
- Clinical outcomes (e.g., acute MI, length of hospital stay)
- Resource utilization (e.g., number of guide catheters, wires, balloons, and stents)
- Discharge to 30-day outcomes
- Surrogate outcomes (e.g., QCA parameters of PCI success, electrocardiographic ischemia, biochemical markers, noninvasive assessment using MRI, a high-intensity signal on the doppler flow wire during PCI, and lumen diameter)
- Clinical outcomes (e.g., acute MI, length of hospital stay, rehospitalization, stent thrombosis, restenosis, and repeat revascularization)
- In-hospital procedural outcomes
- Intermediate (≥30 days to 1 year) and long-term (>1 year) outcomes, including:
- Stent-related outcomes (restenosis, thrombosis, repeat revascularization)
- Surrogate outcomes (cardiac imaging findings [such as ventricular function or myocardial perfusion], electrocardiographic ischemia, biochemical markers, noninvasive assessment using MRI, a high-intensity signal on doppler flow wire during PCI, and lumen diameter)
- Clinical outcomes (MI, death, revascularization or composites of major adverse cardiovascular events, freedom from angina, quality of life, and quality-adjusted survival).
Timing
- Any duration of followup
Study designs of interest
- For diagnostic thinking and therapeutic decisionmaking outcomes, the following study designs will be considered eligible:
- Randomized clinical trials (RCTs)
- Nonrandomized comparative cohort (observational) studies
- Noncomparative cohort studies
- For KQs 1–3 and 5: Studies that compared diagnostic thinking and decisionmaking by applying an IVDx technique in angiographically demonstrated lesions within the same population
- For KQs 4 and 5: Studies that compared diagnostic thinking and decisionmaking by applying two IVDx techniques within the same population
- For process and patient-centered outcomes, the following study designs will be considered eligible:
- RCTs
- Nonrandomized comparative cohort (observational) studies
- No minimum sample size requirement (to be re-evaluated when the literature is being screened; if there are sufficient data from large trials such that adding the smaller trials would not influence the final conclusions, then a minimum sample size will be imposed after consulting with the TEP)
Settings
- Application of IVDx techniques and use in the following settings:
- Tertiary care centers or community hospitals
- In-hospital or stand-alone catheterization laboratories
- Emergent and nonemergent catheterizations
Analytic Framework
Figure 1. Analytic framework for intravascular diagnostic procedures and imaging techniques compared with angiography alone in patients with coronary artery disease
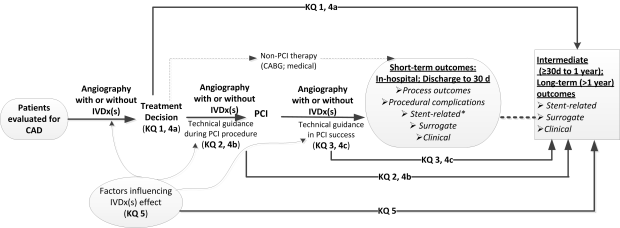
*Undergoing stent implantation.
Abbreviations: CABG = coronary artery bypass grafting; CAD = coronary artery disease; IVDx = intravascular diagnostic technique; KQ = key question; PCI = percutaneous coronary intervention.
This figure depicts the KQs described in the previous section within the context of the PICOTS (population, intervention, comparators, outcomes, timing, study designs, and settings) criteria. In general, the figure illustrates how intravascular diagnostic procedures and imaging techniques—when compared with angiography—may aid treatment decisionmaking during diagnostic angiography, allow procedure optimization and assessment of immediate results in patients undergoing PCI, and improve short-term (in hospital or discharge to 30 days), intermediate (≥30 days to 1 year), and long-term (>1 year) outcomes. Angiography alone is the comparator for KQs 1–3. For KQ 4, the comparator is a different IVDx technique from the index IVDx technique of interest (head-to-head comparisons of IVDx techniques).
Methods
A. Criteria for Inclusion/Exclusion of Studies in the Review
We will use the eligibility criteria for populations, interventions, comparators, outcomes, timing, study designs, and settings (PICOTS) as enumerated above. We do not expect to contact authors for additional data. We will add data from grey literature sources such as Scientific Information Packages from manufacturers, Transcatheter Cardiovascular Therapeutics, the American Heart Association, and the American College of Cardiology and its i2 (Innovation in Intervention) summit conferences. We will eliminate duplicates of published reports. We will extract relevant data and assess methodological quality. If all these studies are of poor methodological quality, then we will conduct sensitivity analyses with and without unpublished studies.
Although the distinction between studies that apply to decisionmaking (KQ 1) versus PCI technical guidance (KQs 2 and 3) is expected to be straightforward, we anticipate that inadequate reporting on the actual timing of the performance of IVDx techniques in certain studies (immediately prior to versus after PCI) may not always render feasible drawing the distinction between studies that belong to KQ2 or KQ3. For example, a study that reports that IVUS-guided stenting was compared to angiography-guided stenting without specifying the timing that IVUS was performed with regards to stent deployment may fall within the scope of both KQ2 and KQ3. Based on clinical consultation with experts, we will assign such studies to the scope of KQ3, since application of IVDx techniques for PCI technical guidance is mostly applied in clinical practice at the “immediately after PCI” time point to evaluate stent deployment results.
B. Searching for the Evidence: Literature Search Strategies for Identification of Relevant Studies To Answer the Key Questions
Appendix Table 1 at the end of this document contains the proposed literature search strategy. We will conduct the search in MEDLINE® and in the Cochrane Central Register of Controlled Trials. We will manually screen all abstracts available in English according to the eligibility criteria, and exclusions will be cross-checked by a second member of the team. The full-text articles of all eligible abstracts will then be reviewed for eligibility. We will tabulate the reasons for excluding any full text articles. For those articles not available in English, we will review the article in its native language, providing someone who has adequate expertise can be identified. A list of articles excluded because of language will be included in the final report. We will ask the internal domain experts to inform us of any potentially missing articles. All suggested articles will be screened for eligibility according to the same criteria used for the original articles. If necessary, we will revise the literature search to find articles similar to those missed. Additional articles will be retrieved from existing guidelines, as well as narrative and systematic reviews. Following submission of the draft report, we will run an updated literature search (using the same search strategy) and will add any relevant articles we find to the final report.
C. Data Abstraction and Data Management
Each study extraction will be conducted by one experienced methodologist and reviewed by at least one other methodologist. Any disagreements will be resolved by discussion in team meetings. Data will be extracted into standard forms in Microsoft® Word. The basic elements and design of these forms will be the same as those we have used for other comparative effectiveness reviews and will include fields that address population characteristics, sample size, study design, analytic details, and outcomes. We will also extract basic demographic data such as age, sex, race, type of index disease (chronic vs. acute CAD), comorbidities, and any other factors that may have a role in modifying the association between the application of IVDx and outcomes. Prior to use, the form will be customized to capture all such elements relevant to the KQs. We will test the extraction form on several studies and revise the form as necessary before full data extraction of all articles is performed.
D. Assessment of Methodological Quality of Individual Studies
We will use methods for evaluating study quality that are standard within the Evidence-based Practice Center (EPC) Program and are recommended by the Agency for Healthcare Research and Quality in the Methods Guide for Effectiveness and Comparative Effectiveness Review, hereafter referred to as the AHRQ Methods Guide.16 Briefly, we will rate each study as being of good, fair, or poor quality based on their adherence to well-accepted standard methodologies. The grading will be outcome specific such that a given study that analyzes its primary outcome well but did an incomplete analysis of a secondary outcome would be assigned a different quality grade for each of the two outcomes. Studies of different designs will be graded within the context of their respective designs. Thus, RCTs will be graded good, fair, or poor, and observational studies will separately be graded good, fair, or poor. However, we expect retrospective studies will likely be of fair or poor quality due to the increased risk of bias inherent in retrospective study designs.
E. Data Synthesis
All included studies will be summarized in narrative form and in summary tables that tabulate the important features of the study populations, design, intervention, outcomes, and results. We will consider performing meta-analyses where there are at least three nonoverlapping studies that are deemed to have sufficiently similar populations, compare the same interventions (i.e., specific type of IVDx technique vs. angiography) and assess the same outcomes. Further analyses will be stratified based on patient- and lesion-level characteristics (diabetes, length of lesion, etc.). We expect to require input from the clinical experts (cardiologists or radiologists) in our team to assess whether studies are too clinically heterogeneous for meta-analysis to be appropriate. We will perform random effects model meta-analyses of continuous, binary, and time-to-event outcomes, as deemed appropriate. The findings of the report will be presented according to the order of the KQs. Within each KQ, findings will be presented separately for diagnostic thinking and therapeutic decisionmaking, as well as for short-term, intermediate, and long-term outcomes. They will be further categorized to specific epochs: in hospital, discharge to 30 days, >30 days to 1 year, and >1 year. Outcome data of interest will include periprocedural complications and process, stent-related, surrogate, and clinical outcomes. Outcome data will be presented in detailed evidence tables and will be summarized in the full text and the executive summary of the report.
F. Grading the Evidence for Each Key Question
We will follow the AHRQ Methods Guide to grade the strength of the body of evidence for each KQ with respect to four domains: risk of bias, consistency, directness, and precision.
Briefly, we will define the risk of bias (low, medium, or high) based on the study design and the methodological quality of eligible studies. We will label the consistency of the data as either “no inconsistency” or “inconsistency present” (or “not applicable” if there is only one study). We do not plan to use rigid counts of studies (e.g., 4 of 5 agree, therefore consistent); instead, we will evaluate the direction, magnitude, and statistical significance of effects across all studies and make a determination. We will describe our logic where studies are in conflict.
We will assess the precision (precise or imprecise) of the evidence based on the degree of certainty surrounding an effect estimate. A precise estimate is an estimate that would allow a clinically useful conclusion. An imprecise estimate is one for which the confidence interval is wide enough to include clinically distinct conclusions—for example, both clinically important superiority and inferiority (i.e., the direction of effect is unknown), a circumstance that will preclude a conclusion.
We will assess the directness (direct or indirect) of the evidence, whether there is a single, direct link between the intervention(s) of interest and the health outcome under consideration. If the studies do not directly compare the tests of interest, we will use network analysis to estimate the comparative effect.
As directed by the AHRQ Methods Guide, we will assign four possible grades for strength of evidence levels: high, moderate, low, and insufficient. These assignments will be based on our level of confidence that the evidence reflects the true effect for the major comparisons of interest.
G. Assessing Applicability
The following factors will be evaluated to assess applicability of study results: age, center characteristics (tertiary vs. community, patient volume, single center vs. multicenter), operator characteristics (e.g., experience), and evaluation of populations with comorbid conditions.
References
- World Health Organization. Cardiovascular Diseases (CVDs). Fact Sheet No. 317. Available at: http://www.who.int/mediacentre/factsheets/fs317/en/print.html. Accessed: August 19, 2011.
- Waxman S, Ishibashi F, Muller JE. Detection and treatment of vulnerable plaques and vulnerable patients: novel approaches to prevention of coronary events. Circulation 2006;114:2390-411. PMID: 17130356.
- Tobis J, Azarbal B, Slavin L. Assessment of intermediate severity coronary lesions in the catheterization laboratory. J Am Coll Cardiol 2007;49:839-48. PMID: 17320741.
- Maehara A, Mintz GS, Weissman NJ. Advances in intravascular imaging. Circ Cardiovasc Interv 2009;2:482-90. PMID: 20031760.
- Casella G, Klauss V, Ottani F, et al. Impact of intravascular ultrasound-guided stenting on long-term clinical outcome: a meta-analysis of available studies comparing intravascular ultrasound-guided and angiographically guided stenting. Catheter Cardiovasc Interv 2003;59:314-21. PMID: 12822148.
- Gerber R, Colombo A. Does IVUS guidance of coronary interventions affect outcome? A prime example of the failure of randomized clinical trials. Catheter Cardiovasc Interv 2008;71:646-54. PMID: 12822148.
- Cantor WJ, Peterson ED, Popma JJ, et al. Provisional stenting strategies: systematic overview and implications for clinical decision-making. J Am Coll Cardiol 2000;36:1142-51. PMID: 11028463.
- Tonino PA, De BB, Pijls NH, et al, for the FAME Study Investigators. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med 2009;360:213-24. PMID: 19144937.
- Hilty KC, Steinberg DH. Vulnerable plaque imaging—current techniques. J Cardiovasc Transl Res. 2009;2:9-18. PMID: 20559964.
- Kushner FG, Hand M, Smith SC Jr, et al. 2009 Focused Updates: ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction (updating the 2004 Guideline and 2007 Focused Update) and ACC/AHA/SCAI Guidelines on Percutaneous Coronary Intervention (updating the 2005 Guideline and 2007 Focused Update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2009;120:2271-306. PMID: 19923169. Erratum in: Circulation 2010;121:e257.
- Smith SC Jr, Feldman TE, Hirshfeld JW Jr, et al. ACC/AHA/SCAI 2005 Guideline Update for Percutaneous Coronary Intervention—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (ACC/AHA/SCAI Writing Committee to Update the 2001 Guidelines for Percutaneous Coronary Intervention). Circulation 2006;113:156-75. PMID: 16391169.
- Orford JL, Lerman A, Holmes DR. Routine intravascular ultrasound guidance of percutaneous coronary intervention: a critical reappraisal. J Am Coll Cardiol. 2004;43:1335-1342. PMID: 15093863.
- Christou MA, Siontis GC, Katritsis DG, et al. Meta-analysis of fractional flow reserve versus quantitative coronary angiography and noninvasive imaging for evaluation of myocardial ischemia. Am J Cardiol 2007;99:450-6. PMID: 17293182.
- Asheikh-Ali AA, Kitsios GD, Balk EM, et al. Vulnerable Atherosclerotic Plaque. Technical Brief No. 3 (Prepared by Tufts Medical Center Evidence-based Practice Center under Contract No. HHSA-290-02-0022). Rockville, MD: Agency for Healthcare Research and Quality; August 2010. AHRQ Publication No. 10-EHC-062-EF.
- Tatsioni A, Zarin DA, Aronson N, et al. Challenges in systematic reviews of diagnostic technologies. Ann Intern Med 2005;142:1048-55. PMID: 15968029.
- Methods Guide for Effectiveness and Comparative Effectiveness Reviews. AHRQ Publication No. 10(11)-EHC063-EF. Rockville, MD: Agency for Healthcare Research and Quality; March 2011. Chapters available at: http://www.effectivhealthcare.ahrq.gov.
Definition of Terms
All terms requiring definition have been addressed in the background and objectives.
Summary of Protocol Amendments
In the event of protocol amendments, the date of each amendment will be accompanied by a description of the change and the rationale.
| Date | Section | Original Protocol | Revised Protocol | Rationale |
|---|---|---|---|---|
|
3/1/2012 |
Key Question 1 |
For patients undergoing diagnostic coronary angiography to evaluate the presence/extent of CAD in order to decide on the necessity for coronary intervention, what is the impact of using an IVDx technique—when compared to angiography alone—on outcomes? |
In patients with CAD, what is the impact of using an IVDx technique and angiography in deciding whether a coronary lesion requires intervention—when compared to angiography alone—on outcomes? |
To improve clarity of the Key Question. |
|
5/1/2012 |
Outcome presentation of Analytical Framework, Methods, and Results section |
Diagnostic thinking, therapeutic decisionmaking, and short- and long-term outcomes |
Therapeutic decisionmaking, intermediate outcomes, and patient-centered outcomes |
To improve clarity of the presentation |
|
5/1/2012 |
All sections |
IVDx |
Intravascular Diagnostic techniques |
Avoid use of unconventional abbreviation |
Review of Key Questions
For all EPC reviews, key questions were reviewed and refined as needed by the EPC with input from Key Informants and the Technical Expert Panel (TEP) to assure that the questions are specific and explicit about what information is being reviewed. In addition, for Comparative Effectiveness reviews, the key questions were posted for public comment and finalized by the EPC after review of the comments.
Key Informants
Key Informants are the end users of research, including patients and caregivers, practicing clinicians, relevant professional and consumer organizations, purchasers of health care, and others with experience in making health care decisions. Within the EPC program, the Key Informant role is to provide input into identifying the Key Questions for research that will inform healthcare decisions. The EPC solicits input from Key Informants when developing questions for systematic review or when identifying high priority research gaps and needed new research. Key Informants are not involved in analyzing the evidence or writing the report and have not reviewed the report, except as given the opportunity to do so through the peer or public review mechanism.
Key Informants must disclose any financial conflicts of interest greater than $10,000 and any other relevant business or professional conflicts of interest. Because of their role as end-users, individuals are invited to serve as Key Informants and those who present with potential conflicts may be retained. The TOO and the EPC work to balance, manage, or mitigate any potential conflicts of interest identified.
Technical Experts
Technical Experts comprise a multi-disciplinary group of clinical, content, and methodological experts who provide input in defining populations, interventions, comparisons, or outcomes as well as identifying particular studies or databases to search. They are selected to provide broad expertise and perspectives specific to the topic under development. Divergent and conflicted opinions are common and perceived as health scientific discourse that results in a thoughtful, relevant systematic review. Therefore study questions, design and/or methodological approaches do not necessarily represent the views of individual technical and content experts. Technical Experts provide information to the EPC to identify literature search strategies and recommend approaches to specific issues as requested by the EPC. Technical Experts do not do analysis of any kind nor contribute to the writing of the report and do not have the opportunity to review the report, until the public review period.
Technical Experts must disclose any financial conflicts of interest greater than $10,000 and any other relevant business or professional conflicts of interest. Because of their unique clinical or content expertise, individuals are invited to serve as Technical Experts and those who present with potential conflicts may be retained. The TOO and the EPC work to balance, manage, or mitigate any potential conflicts of interest identified.
Peer Reviewers
Peer reviewers are invited to provide written comments on the draft report based on their clinical, content, or methodological expertise. Peer review comments on the preliminary draft of the report are considered by the EPC in preparation of the final draft of the report. Peer reviewers do not participate in writing or editing of the final report or other products. The synthesis of the scientific literature presented in the final report does not necessarily represent the views of individual reviewers. The dispositions of the peer review comments are documented and will, for CERs and Technical briefs, be published three months after the publication of the Evidence report.
Potential Reviewers must disclose any financial conflicts of interest greater than $10,000 and any other relevant business or professional conflicts of interest. Invited Peer Reviewers may not have any financial conflict of interest greater than $10,000. Peer reviewers who disclose potential business or professional conflicts of interest may submit comments on draft reports through the public comment mechanism. It is our policy not to release the name of the Peer reviewers of TEP panel members until the report is published so that they can maintain their objectivity during the review process.
Appendix Table 1
| # | Searches | Results |
|---|---|---|
| 1 | intravascular.af. | 38,643 |
| 2 | intra-vascular.af. | 214 |
| 3 | endovascular.af. | 25,071 |
| 4 | endo-vascular.af. | 19 |
| 5 | endocoronary.af. | 39 |
| 6 | endo-coronary.af. | 4 |
| 7 | intra-coronary.af. | 185 |
| 8 | intracoronary.af. | 9,142 |
| 9 | endoluminal.af. | 3,133 |
| 10 | endo-luminal.af. | 12 |
| 11 | transluminal.af. | 14,433 |
| 12 | trans-luminal.af. | 26 |
| 13 | intraluminal.af. | 12,938 |
| 14 | intra-luminal.af. | 232 |
| 15 | 1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11 or 12 or 13 or 14 | 9,8862 |
| 16 | magnetic resonance imaging.af. | 266,900 |
| 17 | magnetic resonance angiography.af. | 15,166 |
| 18 | exp magnetic resonance imaging/ | 247,897 |
| 19 | exp magnetic resonance angiography/ | 13,548 |
| 20 | elastography.af. | 1,307 |
| 21 | thermography.af. | 6,794 |
| 22 | microcirculatory resistance.af. | 32 |
| 23 | vascular resistance.af. | 52,884 |
| 24 | thermodilution.af. | 4604 |
| 25 | exp Thermodilution/ | 2209 |
| 26 | hemodynamics.af. | 137,391 |
| 27 | exp Hemodynamics/ | 557,384 |
| 28 | exp endosonography/ | 7,125 |
| 29 | physiologic measurement*.af. | 316 |
| 30 | doppler ultrasound.af. | 9,280 |
| 31 | coronary pressure.af. | 474 |
| 32 | doppler velocimetry.af. | 1,916 |
| 33 | ultraso*.af. | 345,127 |
| 34 | 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28 or 29 or 39 or 31 or 32 or 33 | 1,134,074 |
| 35 | 15 and 34 | 25,039 |
| 36 | exp coronary angiography/ | 43,276 |
| 37 | ultraso$.af. | 345,127 |
| 38 | ffr.af. | 739 |
| 39 | fractional flow reserve.af. | 563 |
| 40 | coronary flow reserve.af. | 1,705 |
| 41 | coronary flow velocity reserve.af. | 301 |
| 42 | angioscop$.af. | 1,642 |
| 43 | optical coherence tomography.af. | 7,755 |
| 44 | exp Tomography, Optical Coherence/ | 7,570 |
| 45 | blood flow velocity.af. | 50,905 |
| 46 | exp Blood Flow Velocity/ | 48,793 |
| 47 | doppler flow wire.af. | 138 |
| 48 | pressure wire.af. | 120 |
| 49 | coronary pressure measurement.af. | 24 |
| 50 | exp endosonography/ | 7,125 |
| 51 | 37 or 38 or 39 or 40 or 41 or 42 or 43 or 44 or 45 or 46 or 47 or 48 or 49 or 50 | 390,940 |
| 52 | 36 and 51 | 6,029 |
| 53 | exp Ultrasonography, Interventional/ | 11,033 |
| 54 | exp Fractional Flow Reserve, Myocardial/ | 215 |
| 55 | fractional flow reserve.af. | 563 |
| 56 | intravascular ultrasound.af. | 4451 |
| 57 | IVUS.af. | 2405 |
| 58 | 53 or 54 or 55 or 56 or 57 | 13,349 |
| 59 | 35 or 52 or 58 | 36,060 |
| 60 | exp myocardial ischemia/ | 333,632 |
| 61 | exp Angioplasty, Transluminal, Percutaneous Coronary/ | 28,041 |
| 62 | exp stents/ | 42,961 |
| 63 | exp Angioplasty, Balloon, Coronary/ | 28,040 |
| 64 | exp Myocardial Revascularization/ | 74,441 |
| 65 | exp drug-eluting stents/ | 3,317 |
| 66 | 61 or 62 or 63 or 64 or 65 | 106,646 |
| 67 | 60 and 66 | 54,147 |
| 68 | 59 and 67 | 4,131 |
| 69 | remove duplicates from 68 | 3811 |
| 70 | exp animals/ not humans.sh. | 3,582,822 |
| 71 | 69 not 70 | 3,721 |